
As perceptions among lawmakers and medical professionals shift toward seeing the current heroin epidemic as a public health crisis, policies are slowly falling into place that are aimed at saving lives. But despite these efforts and recognition of the problem being bigger than something a law enforcement first approach can address, addiction continues running rampant.
From a dollars and cents perspective, the cost is staggering. A 2011 study from the U.S. Department of Justice’s National Drug Intelligence Center (NDIC) looked at the economic impact of drug addiction in terms of medical care, lost productivity and crime on a national level. For the year 2007, the NDIC estimated that the cost of illicit drug use totaled more than $193 billion.
But there is more at stake here than money. Perhaps the biggest cost being paid comes from families who have lost their loved ones to death, imprisonment or simply a life spent prioritizing a fix over the people who care about them. From the cell block to the maternity ward, this epidemic has a human cost that simply can’t be overlooked or accurately calculated.
In order to prevent additions to the already horrifying statistics related to this epidemic, America has to address its addiction problem from all angles.
You Might Also Enjoy: Did you miss Part 2: Needles in the Haystack? Be sure to read it here!
The Road to Recovery
What inspires people to get clean differs depending on the individual. For some, it’s seeing their friends or someone they love die. For others, it’s the erosion of their relationships or the failure of their career. For Dayton, Ohio’s Jeremiah Hess, it was a run-in with the law that made him reconsider his future.
In April 2010, the then 41-year old was shown in security camera footage by a local news station after he stole a woman’s purse and tried to use her credit cards at a gas station. He was identified by a correctional officer who recognized him while watching the footage, and then called the police. In the end, it was the wakeup call Hess needed as he began to realize something important.
“It wasn’t taking the pain away anymore,” Hess said. “I’d go harder and harder and eventually you either die or somebody helps. By then, I lost everything. I had nothing. I lost my family, everything. I went to jail, they put me through a program and there I met a counselor. She helped me get rid of some of my anger, helped me forgive people and get past things that I had been struggling with.”
Ultimately, getting past an addiction is a physical and psychological battle. The latter can be a long-term struggle that many addicts never stop fighting.
“It’s difficult because you have to get down to what’s driving the addiction,” Hess said. “What is the pain that drives it? There’s something. Everybody is different, but you have to deal with what’s going on inside of you. You can get past the physical part with being sick, but then you have to deal with why you still want to get high.”
Getting There Before It’s Too Late
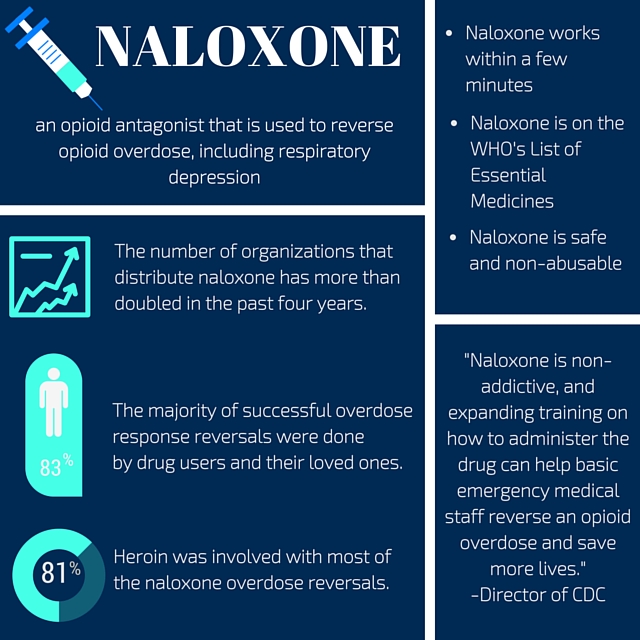
Overdose death numbers are shocking, but they could, in fact, be a lot worse if not for the proliferation of naloxone (pronounced nuh-lox-ohn), often referred to by its brand name – Narcan.
Delivered intravenously or via nasal spray, naloxone is a powerful opiate antagonist that almost instantaneously reverses the effect of an opiate overdose. The drug is now being delivered in record doses and distributed to law enforcement professionals, school nurses, paramedics and users’ families in states all around the country.
The Centers for Disease Control and Prevention recommended in 2015 that lawmakers expand the definition of who can administer the drug legally without fear of liability consequences. In many states, only advanced EMS personnel can administer the drug via injection, while the nasal version of the drug can be administered by anyone with training.
The drug is non-addictive and expanding its use can save lives, particularly in rural areas where the CDC estimated overdose deaths from heroin and prescription opiates to be 45% higher than in cities. The drug is not new, having been approved by the Food and Drug Administration in 1971 as an injectable to be used primarily in hospitals.
But there are problems with expanding the use of naloxone, primarily the price. Because of increased national demand, the primary manufacturer of naloxone, Amphastar Pharmaceuticals, has doubled the price, citing increased manufacturing costs. Amphastar is currently the only company that makes the intranasal version of naloxone, which at present isn’t approved by the FDA.
According to the National Conference of State Legislatures, more than 150,000 “laypeople” received naloxone training and had been given rescue kits nationwide by November of 2015, resulting in 26,000 reported overdose reversals.
Cities around the country now have to assess the cost of Narcan, estimated at around $40 per dosage, according to a September 2015 story from National Public Radio. They also need to examine the Good Samaritan laws that you might expect to accompany any type of policy surrounding the drug.
In an effort to encourage people to seek medical help or follow up treatments for overdose victims after naloxone has been used successfully, 34 states and Washington D.C. have enacted some form of immunity laws. These laws protect 911 callers seeking help for overdose victims from being charged with low-level drug possession or use offenses. This does not extend to seeking help during the course of an arrest, however.
Other requirements for attaining immunity in this situation include remaining on scene until help arrives and cooperating with emergency personnel.
But another problem with the drug persists; naloxone is not a cure for heroin addiction. It is simply a lifesaving drug in the case of overdoses. Immediately following a naloxone revival is a good time to address one’s addiction, but healthcare workers told NBC News in 2014 that opportunities are often missed by a “patchwork healthcare system.” Patients walk out of the hospital after being revived, with a list of treatment options on their discharge papers, but little else is done to motivate or push them in the right direction.
Planting the Seeds
Getting an addict off of opiates often takes a number of efforts. Increasing the number of exposure points to people who can help start them down the path to recovery is often a key part of the journey. In part one of our series, we met a 32-year-old recovered heroin user from Dayton, Ohio who wished to remain anonymous. In sharing his story with Healthcare Daily Online, he identified his early exposure to mandated treatment as one of the biggest reasons he decided to get clean.
“The first two times were mandated outpatient treatment sessions, and my heart wasn’t in it,” he said. “I was bitter about being there, and I thought many of the counselors and people in recovery were full of crap. But I did retain some of the stuff I heard, and it did contribute to my eventual decision to try a 12-step program.”
Numerous exposures to programs is not always easy, however, as not every addict winds up in a state-mandated treatment facility. Reaching out to addicts earlier is a growing priority, and with President Obama seeking $1.1 billion to combat this addiction crisis with expanded treatment programs, there has never been a better time to connect with addicts and attempt to get them help. But how?
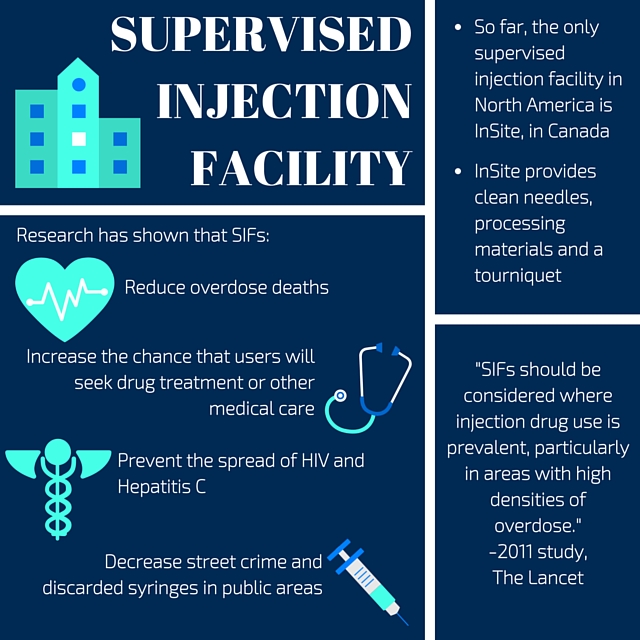
One idea that is picking up traction in Seattle and throughout parts of Canada is that of the supervised injection facility (SIF). By supplying addicts with fresh needles and safe, secure places to shoot up, advocates of SIFs say they can minimize the spread of viruses such as HIV and Hepatitis C in the injection drug user (IDU) population. These facilities provide windows of time to talk to users about their life in an attempt to plant the seed of desire for something better, and have also proven effective in preventing overdose deaths.
Safe injection sites are not currently open in the U.S., but are a sort of cousin to needle exchange programs that already exist to allow IDUs to turn in used needles for new clean ones. The precedent for these facilities, which are set to open in Montreal, Canada this year, comes from another north of the border locale, Vancouver, B.C.
Canada’s western province implemented North America’s first SIF called InSite in 2003. It has been greeted with a mix of criticism and praise that makes it tough to gauge its effectiveness at times. Critics say that despite all of InSite’s claims, it’s just another place to get high, and government resources ought to be used to fund treatment and recovery facilities.
But according to a report from the British Columbia Centre for Excellence in HIV/AIDS and doctor’s from St. Michael’s Hospital in Toronto, SIFs are effective in lowering the burden placed on the healthcare system. Doctors treat fewer HIV and Hepatitis C infections, and the sites are safe for users, who are monitored, as this greatly reduces the possibility of an overdose death.
Using InSite as a baseline, the Montreal Gazette reported that St. Michael’s researchers estimated that one location in Toronto would incur $33.1 million in operating expenses over a 20-year span, but save $42.7 million in healthcare costs. That’s because they estimated a single site would prevent 164 HIV infections and 459 Hepatitis C infections.
According to an article from the National Library of Medicine, titled “The Law and Politics of Safe Injection Facilities in the United States,” Vancouver’s SIF has reduced needle sharing and overall syringe usage. The facilities also provide clean water for injecting, lead to less outdoor injections and offer the proper equipment for processing and filtering the drugs.
The way it works is pretty simple. InSite does not provide the narcotics; addicts show up at the facility with drugs acquired on the street. They are given the items necessary to consume the drug, including clean needles, processing materials and a tourniquet, and are provided a booth to take the drugs in. While there, they are monitored by medical staff in case of an overdose, and if they express interest in getting help, they are connected with services that can help them find treatment centers.
According to a 2011 study from The Lancet, InSite’s creation correlated with a large drop in drug deaths in the surrounding areas. InSite’s website boasts that despite having seen more than 1,000 overdose cases, there has never been a single death in their facility. The Lancet study concluded that “SIFs should be considered where injection drug use is prevalent, particularly in areas with high densities of overdose cases.”
Seattle is lining up to be the first SIF location in the United States, according to an article from Seattle Weekly. There are plenty of opponents to this idea, the legality of which is questionable. But there are other options on the table that don’t necessarily imply allowing people to get high and are more focused on helping addicts get treatment.
Did you miss it?: American Heroin Part 2: Needles in the Haystack
Law Enforcement Assisted Diversion (LEAD)
Seattle’s problem with heroin runs throughout the city and suburbs. A study from the University of Washington’s Alcohol & Drug Abuse Institute showed that fatal heroin overdoses increased by 58% in 2014, totaling 156 lives taken. This has led to an increase in treatment-based approaches to fighting the epidemic in an attempt to interrupt what has become a cycle of arrests, prosecutions and incarcerations for many non-violent drug offenders.
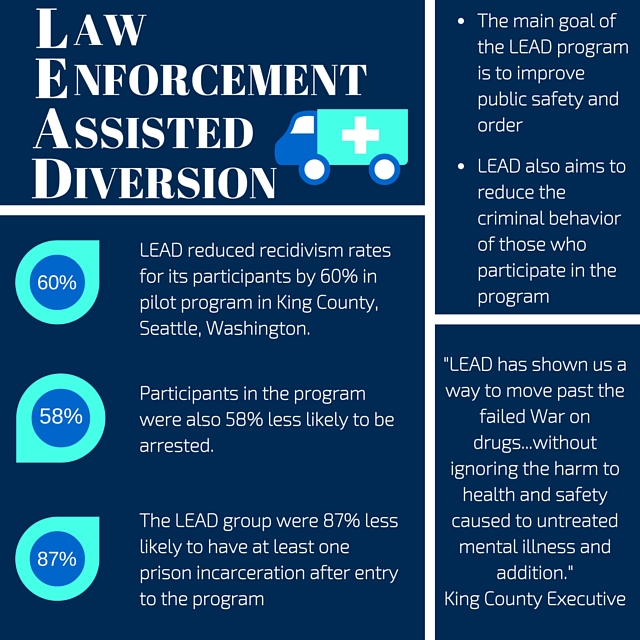
One idea to disrupt the cycle is that of law enforcement assisted diversion (LEAD). Launched as a four-year pilot project in 2011, the program has exceeded expectations in terms of its success. LEAD offers drug offenders that have been arrested the chance to work with a case worker who can provide immediate help, be it a warm meal or safe place to sleep, as well as long-term drug treatment services and job training, rather than face potential jail time.
LEAD is only offered under the conditions that the subject volunteers to participate, is not carrying more than three grams of narcotics at the time of arrest, has no felony convictions for violent crimes and is not suspected of prostitution or exploiting minors in drug dealing operations.
An evaluation by the University of Washington revealed that compared to a control group, LEAD reduced recidivism rates for its participants by 60%. The project is based on what is known as a harm reduction model that has come out of decades of public health research. The success of the program has many calling for it to be replicated in other parts of the country. Santa Fe, New Mexico launched its own version of LEAD in 2014, while Albany, New York plans to do the same in 2016.
Other cities that are taking the measure under consideration include San Francisco, Atlanta, Houston and Portland, Maine according to an article from the Huffington Post.
In Massachusetts, Gloucester Police Chief Leonard Campanello grew so tired of watching the cycle lead to overdose deaths that he took matters into his own hands, posting on the department Facebook page offering addict’s an alternative. Provided they turn in their stash and agree to receive treatment, the department would not arrest them, but point them in the direction of treatment centers and even help them get financial help to pay for it. In the first 90 days, 145 people took advantage of Campanello’s offer, according to Boston Magazine.
The Wait for Rehab
As America’s opiate dependency shifted from crisis to epidemic in the national consciousness, treatment centers looking to help people were overrun by large numbers of addicts looking for help. While heroin users coming to the realization they need to get clean before a grim inevitability occurs is ultimately positive, it doesn’t do much good when they can’t find help.
According to a 2015 story from NBC News, wait times around the country for addicts are increasing as federally funded rehab opportunities fall short. In Massachusetts, the wait can be weeks. In Florida, months may go by. In Maine, wait times have been as long as 18 months.
It’s easy to say addicts should fund their own rehab, but in most cases that is not realistic.
[pullquote align=”full” cite=”” link=”” color=”” class=”” size=””]According to the Huffington Post, the average price of privately funded residential rehab is approximately $31,500 per month.[/pullquote]
The treatment addicts do receive is often inadequate, with many facilities prioritizing an abstinence-only approach to treatment. That, however, fails to address the changes in brain function that can occur within a person over long periods of opiate use. For that, specific treatment using medication is often needed.
A 2012 study from the National Center on Addiction and Substance Abuse at Columbia University recommended an overhaul of the country’s treatment system and called the low-level care addicts receive “a form of medical malpractice.”
The consequences from this are dire to say the least, with families of the addicted suffering the most. In Maine, where wait times for rehab facilities are the longest, the past three years have seen a 58% increase in child abuse and neglect cases. The number of drug-affected newborns has increased by 600%. This is a national trend.
According to an article from Reuters, a baby is born dependent on opiates every 19 minutes in the United States. Looking at hospital discharge records, Reuters found more than 27,000 diagnosed cases of drug dependent newborns in 2013 alone.
This type of drug dependency is known as neonatal abstinence syndrome. The child, suffering withdrawals from not receiving the drugs its mother provided while in the womb, requires weeks of therapy. They are often unable to sleep, suffer muscle contractions in their arms and legs and experience heavy sweating and acidic diarrhea.
According to an article in the Washington Post, there is a significant economic cost associated with the treatment of these newborns as well, averaging $53,000 per patient.
Sadly, after many of these newborns survive being weaned off the drugs, they are sent home with addicted mothers incapable of caring for them. The Reuters article identified 110 cases since 2010 in which babies who were born drug dependent recovered and were discharged from the hospital, only to die preventable deaths in the weeks and months that followed due to negligent parenting.
Changing the Tide
One of the biggest assets in battling this epidemic is people. While there aren’t enough beds to treat the volume of addicts seeking help, there is yet another problem; the amount of qualified people to help treat them.
As government funds increase the amount of facilities available to addicts, the problem of staffing is going to be a big issue. The healthcare industry in general is struggling to maintain the necessary workforce to help care for the aging Baby Boomer generation, a group that makes up the majority of current healthcare workers. Add to that the increased demand surrounding addiction treatment, and the American healthcare system may be facing a full blown personnel crisis.
And it isn’t just nurses either. It’s all across the spectrum of care, from administrators to manage facilities, to counselors and IT professionals involved in implementing new technology into the field.
If you are interested in saving lives by being an active participant in the battle against addiction, there are career fields you can enter to help you do just that. Whether you are a current healthcare professional looking to switch fields or a concerned citizen wanting to help steer people’s lives in a positive direction, one of these positions can provide a fulfilling career centered around fighting this epidemic.
Careers
Healthcare administrator: Treatment centers have logistical needs just like other medical facilities. This falls under the work of an administrator, whose job is to coordinate medical services, handle medical records and create work schedules for employees. They also need to be up-to-date on the latest technology and laws concerning their branch of healthcare, while playing an important role in the overall execution of care. Most healthcare administrators hold at least bachelor’s degree.
Healthcare manager: Rehabilitation, particularly residential rehab, in which patients live at the facility for a period of time, can be costly to both patient and facility. Insurance policies, funding, understanding healthcare policy and anything having to do with the business aspect of running a facility fall under the stewardship of a healthcare manager. In most cases, healthcare managers hold a master’s degree.
Substance Abuse Counselor/Addiction Specialist (Psychology): “She superman punched my wall that was keeping all this stuff inside. I let her peek inside and told her things that I had never told anybody. I trusted her and she kept digging. And eventually she helped me get to what was driving my addiction,” said now 47-year old Jeremiah Hess.
This type of testimony is not uncommon from recovered addicts like Hess. Drug counselors are key players on the front lines of this battle by helping users break the psychological bond to heroin that is the root cause of so many relapses.
This does require some education, most commonly in psychology. A study conducted by the Substance Abuse and Mental Health Services Administration found that 75% of addiction counselors hold at least a bachelor’s degree.
Substance Abuse Nurse: Nurses are key players in the spectrum of care regardless of the healthcare setting, and addiction rehabilitation is often no different. Getting people through the physical pain of withdrawals and into recovery is as much a medical process as it is mental. Also referred to as addiction nurses, these professionals specialize in pain management and at times, behavioral psychology. Any registered nurse is eligible for this position, but leadership skills are often a necessity. An RN to BSN program can prove beneficial to someone dedicated to working in this field.
Law enforcement: A career in law enforcement is intrinsically tied to fighting this epidemic. This can include investigating drug-related crimes, implementing diversion programs or working as an agent in the Drug Enforcement Administration or the U.S. Department of Homeland Security: Customs and Border Protection. In any case, meaningful work that goes beyond arresting low-level offenders and paroling the streets means moving up in the ranks, which requires a minimum of a bachelor’s degree.
Social worker: Substance abuse social workers are assigned on a per case basis and help identify the needs of a person recovering from addiction, whether it’s helping them find housing or work, reconnecting with their families or meeting personal goals. Between 2014 and 2024, employment of social workers is expected to grow by 12%, according to the U.S. Bureau of Labor Statistics. The majority of social workers hold at least a bachelor’s degree, though some clinical settings may require a master’s degree.
Drug Informatics: Given heroin’s spread to even the most rural areas of the country, having treatment centers that serve addicts in all areas is not realistic. Because of this, the growing field of telehealth is about to get even bigger. In 2014, the U.S. Bureau of Justice Assistance awarded a $100,000 grant to the South Dakota Department of Social Services to determine how to implement telehealth services that connect treatment providers with patients that live in rural areas.
Using a computer, outpatient services can be provided as well as support services. In Houston, Memorial Hermann Health System’s Prevention and Recovery Center (PaRC) uses a 24/7 support platform called OneHealth that provides online support groups to people in after-care, the portion of recovery after a person exits a treatment center. Implementing, operating and maintaining these systems, however, is no small task. A degree in healthcare informatics can help individuals streamline these programs and push the field of informatics into reorganizing the way healthcare is delivered.







{kind=link}